Unlock a world of possibilities! Login now and discover the exclusive benefits awaiting you.
- Qlik Community
- :
- Forums
- :
- Groups
- :
- Industry and Topics
- :
- Healthcare
- :
- Wu's News - Operating Room Efficiency
- Subscribe to RSS Feed
- Mark Topic as New
- Mark Topic as Read
- Float this Topic for Current User
- Bookmark
- Subscribe
- Mute
- Printer Friendly Page
- Feature this Topic
- Mark as New
- Bookmark
- Subscribe
- Mute
- Subscribe to RSS Feed
- Permalink
- Report Inappropriate Content
Wu's News - Operating Room Efficiency
Howdy folks! My name's Jeff Wu, and I'm a Solutions Architect here at QlikTech. I joined QlikTech back in June of 2012 and prior to that was at Epic for six years serving as the Senior Application Director for the OpTime and Anesthesia applications.
Since joining I've gotten an opportunity to see what a lot of customers are doing with Qlikview and it has sparked my passion for better healthcare delivery and a desire to share my experiences in healthcare with others.
Today I'd like to talk about my favorite place in the hospital…
The Operating Room.

You're getting sleepy...
In my years as an implementer, I've gone live with Epic at over 50 individual hospitals; there really is no place like the ORs. With the ED a close second, there is no place in the hospital that is more critical to have operational efficiency from start to finish. According to a recent HIMSS article, the ORs are responsible for up to 60% of a hospital's revenue. On that note, the ORs can also account for more than 60% of a hospital's margin. This means that the most minor of problems in this area can have monumental effects on a hospital's operational effectiveness. First Case Late Starts, Delays, Add-on Cases, PACU time, patient transfers, etc. can all have very negative repercussions if not addressed in a timely fashion.
Take for example, the effect of one situation:
A surgeon is 15 minutes late to pre-op his first patient of the morning. The patient is scheduled for a basic laparoscopic cholecystectomy to treat gall stones. When she arrives, the surgeon speaks with the anesthesiologist, who is hesitant to go through with the procedure due to the patient's history of smoking, asthma, diabetes, and a recent bout of pneumonia. The surgeon is annoyed, but not wanting to lose her surgical slot, orders some STAT blood tests to check the patient's ability to undergo surgery. Upon return, it is confirmed that the patient is too sick to undergo the procedure. The case is cancelled.
What sort of revenue impact did this have? Well let's see. Due to the surgeon arriving late, the case was cancelled too late to actually make use of the room time. Both the surgeon and anesthesiologist lost the revenue that would be associated with performing the procedure. To insure speedy transitions, supplies for a surgery are laid out prior to a patients transfer into the OR--all those supplies are now wasted. Any pre-induction meds mixed specifically for that patient by the pharmacy or anesthesiologist are also wasted. What started as one small problem (surgeon arriving late) can develop into a significantly more complex problem. Now, you might think that this is a very rare occurrence that such an unfortunate series of events could happen, but I guarantee that if you talk to any surgical staff, this kind of thing has happened at least once in the past month, or more probably, the past week.
All of these combine for a massive loss to the hospital. Now, there are bound to be times when physicians are late; there are bound to be times when a patient forgot that they had to be NPO, but addressing what can happen will mitigate the financial impact of what inevitably will happen.
So how can we address this?
With data.
But not just any, or some, we need all of it. All of it is the only way we can have an informed understanding of the situation and make an informed decision to correct it. As technology has progressed, sophisticated documentation systems have evolved to capture all the components that are necessary to address these problems. The next problem is that this data lies in disparate systems that have difficulty communicating with each other. This was what I dealt with on a near daily basis in my time at Epic. Customers came to me with problems that they had the data to understand and correct but could not associate it meaningfully to make an informed decision. Take, for example, the very simple question every OR Director or Manager has to deal with:
Based on the number of add-on cases for the day, should I open an additional OR or pay my staff overtime?
This seems like a simple question, but what goes in to making an informed decision for an issue like this is extremely complicated. Factors such as the add-on procedures, to the staff on hand, to the cost of staff, average hours per stay, average time per procedure, even the day of the week can all impact whether the person in charge says yay or nay to something as simple as opening an additional OR. Additionally, this information is in multiple places besides the EMR. In my experiences prior to QlikView, OR Directors and managers were relegated to simply making gut checks on whether they thought a new OR was needed or whether paying staff overtime was sufficient, even though they had powerful systems and loads of data to look across to make a decision.
Here's where I get excited by QlikView. Because of QlikView's inherent powers to associate disparate sources of data, the previously difficult or impossible is now a logical first step.
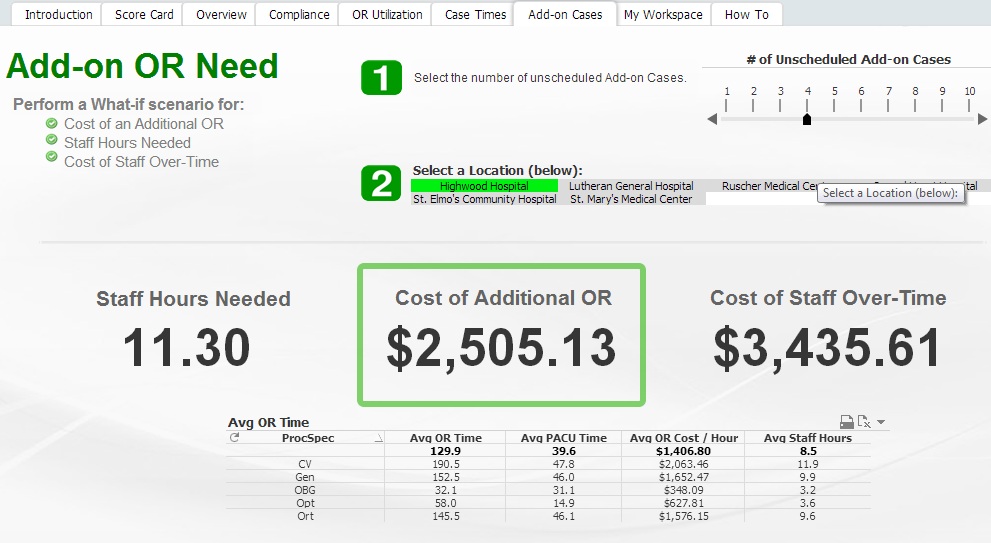
This application takes into account EMR and Timelog data to help visualize information for decision making.
And we're just scratching the surface on what's possible.
Check out our upcoming marketing data sheet on ED and OR operational efficiency coming soon!
Up Next: A review of Meaningful Use Stage I and a foray into Meaningful Use Stage II
- Tags:
- Group_Blogs
- Mark as New
- Bookmark
- Subscribe
- Mute
- Subscribe to RSS Feed
- Permalink
- Report Inappropriate Content
Jeff
I have already received positive feedback regarding your blog from a CMIO in New England and 2 Quality Improvement Analysts. Direct quote from one of the analysts:
"Thank you for sharing this wealth of resource."
They're looking forward to your next post on MU Stage I & II.
Keep up the great work and the continued dedication to our provider & payor customers in the Healthcare Industry.
Cheers,
Chris
- Mark as New
- Bookmark
- Subscribe
- Mute
- Subscribe to RSS Feed
- Permalink
- Report Inappropriate Content
Hi Jeff,
I was looking for an example of a Peri Operative Dashboard. I stumbled on your Blog/Notes. I'm certified in Optime and Anesthesia. I started on Mckesson Surgical Manager and Scheduling System. I made a career change. I'm now an Analytics Developer. We are using Qlik Sense. Can you please share how you implemented Block Utilization in Qlik. What are the KPI or measures you implemented for block utilizations? Thanks!